Cómo citar este artículo: López García, R. A., Barragan Lordoño, M. J., & Vargas Aguilar , I. (2021). Detection and clinical impact of anxiety in Children undergoing general anesthesia compared to the standard of care of a pediatric hospital.: Detección e impacto clínico de la ansiedad en niños sometidos a anestesia general en comparación con el estándar de atención de un hospital pediátrico. Revista Electrónica AnestesiaR, 13(10). https://doi.org/10.30445/rear.v13i10.1016
Resumen en castellano: Detección e impacto clínico de la ansiedad en niños sometidos a anestesia general en comparación con el estándar de atención de un hospital pediátrico.
Introducción: El impacto de la ansiedad preoperatoria provoca dolor posoperatorio significativo, delirio, alteraciones del sueño y otros cambios conductuales desadaptativos que duran semanas o meses después de la cirugía.
Método y resultados: se realizó un estudio observacional, transversal y descriptivo en 97 niños de 7 a 10 años sometidos a cirugía electiva. Se les aplicó la escala de ansiedad manifiesta en niños (CMA-R), se utilizaron frecuencias, porcentajes y pruebas cruzadas para encontrar factores asociados a la ansiedad. Los resultados se comparan significativamente con la literatura, presentando ansiedad en el 52,5% de los pacientes, donde el nivel socioeconómico influye en que esto ocurra.
Conclusiones: Los resultados del estudio demuestran que la escala es útil y atractiva para detectar la ansiedad preoperatoria en niños sometidos a cirugía ambulatoria en comparación con el protocolo de atención estándar en los hospitales pediátricos.
López García RA (1), Barragán Lordoño MJ (2), Vargas Aguilar I (2)
(1) Pediatric anesthesiologist. Centenario Hospital Miguel Hidalgo, Aguascalientes, México.
(2) Pediatric anesthesiologist. Instituto Nacional de Pediátrica, México DF, México.
Introduction
There is no time or place recorded in history where fear and anxiety are not part of human existence, fear of the harmful or incidents that occur in life as an adaptive response for the human species. In the pediatric age, anxiety can be so injurious that it cannot make appropriate decisions or actions to solve a problem, inappropriate behavior, or constitute a non-adaptive response to the environment. 1
In the life of a person especially in a child and his family, being subjected to hospitalization, surgery or an anesthetic procedure are events of high impact for the rest of his life, due to the long-term psychological effects and their consequences in behavior, particularly in the pediatric patient, between 40% and 60% of cases to experience high levels of anxiety on the day of surgery, and more than 30% moderate to severe postoperative pain. 2 Anesthesia, especially in the phase of the Induction, can be a stressful period that is associated with increased risk of psychological and behavioral changes, being observed in three different aspects; Preoperative anxiety, delirium and changes in post-operative behavior, especially of the negative type such as sleep disorders, eating disorders, separation anxiety, tantrums, aggression towards the authorities that can occur in up to 50 to 60% of all children undergoing general anesthesia. 2-3
Brazilian authors performed preoperative evaluations in scheduled outpatient surgery, finding a high prevalence (81.6%) of anxiety among children (4.67 ± 0.96 years) . 4 The ages between 4 and 8 years prevailing between 38.9% to 84% was observed in the waiting room, patients with preoperative anxiety are three times more likely to exhibit negative behaviors.
In 2011, Yuki identified the association of unsatisfactory anesthesia and aggressive behavior in 612 minors undergoing otolaryngology surgery, this led to the importance of addressing anxiety in the perioperative period. 67% of the cases have negative conduct after surgery, 45% presented it on the second day, 23% at two weeks after surgery; however these changes could persist for up to 6 months in 20% and one year in 7.3% of them, affecting the responses of subsequent medical care and socialization in school. 5
There are risk factors strongly related to preoperative childhood anxiety, it has been shown that a reduction in them has been shown to minimize stress in 25% of patients. 6-7 Unfortunately, a recent survey shows that currently most medical staff, do not detect them.
Parental anxiety is the risk factor that is most associated between the child’s anxiety and negative behavioral changes.8 Language, discrimination and stress caused by parents may be involved in the presence of psychological distress.8-11 Karling and Hägglöf 12 reported that the education level of the parents acts as a factor of protection against general anxiety, an explanation could be the ability of a highly educated mother to have a better understanding of the harmful aspects, complications or benefits related to surgery. Since 2000 there are preoperative programs in the literature that consists of written and modeled information together with the child and his parents, to give the exact information; However, it is not commonly used in hospitals because of the high economic cost or lack of assistance from family members. 13
It was noted that both pain and anxiety work in a similar mechanism, postoperative pain activates the sympathetic nervous system, which stimulates the hypothalamus to release neurotransmitters such as adrenaline and norepinephrine; affecting alertness, persisting up to 4 weeks after surgical event.14 Supported by Kain (2006) who revealed that most anxious individuals tend to take more doses of pain relievers, have sleep problems and emotional disorders.15
Kotiniem (1997) conducted a cohort study with 3 and 12 years old patients scheduled for anesthesia in a variety of procedures found that one of the factors causing anxiety and negative behavior was bad experiences with previous past methods, memories negatives of previous hospital experience, visit the pediatrician or dentist. 16 Fortier and Martin17 reported that surgical or medical histories might worsen or minimize anxiety, depending on the quality of the anesthetic event.
Age is a factor that interferes with the appearance of anxiety in the preoperative period, in the pediatric population the perception of the anxiety phenomenon also depends on the stage of development and the cognitive potential of the child, since different responses were observed between those who face the same stress factor. 18-19 Preschoolers can relate anxiety to physical symptoms in the face of imminent surgery, children seek explanations for the situation because they have fears about surgery.19 While schoolchildren, with more advanced cognitive development can be involved in decision making, and feeling of fright, no doubt lies in the possibility of not recovering from anesthesia. Therefore, the child must be treated and understood individually, taking into account the stage of development in which he is.
Regarding socioeconomic status level and anxiety, associations have not been significant, however, in the upper class the physical and psychological conditions of the children effectively face stressful situations, such as surgery.20-21 An investigation of the University of Goiania, Brazil,22 210 cases interviewed in the waiting room were recruited, anxiety was assessed by the modified Yale scale, in which it is concluded that 42% of children presented nervousness with associated factors such as age between 5 to 6 years and middle-upper socioeconomic class with significant results. 22
Objective
The objective of this research was to evaluate the detection and clinical impact of anxiety in children determined by frequency, compared to the standard of care in a pediatric hospital.
Material and method
The investigation was carried out at the National Institute of Pediatrics, Mexico City between July 2017 and January 2019. A prospective, cross-sectorial, descriptive study was carried out; after obtaining the approval of the ethics committee of the institute, a written consent has been given to participating parents and sons for the preoperative evaluation of psychometric parameters.
The patients to choose were pediatrics scheduled for elective and outpatient surgery between the ages of 7 to 10 years, Mexicans with a physical state of The American Society of Anesthesiologists (ASA) I-II, to undergo general anesthesia. Those patients with ASA III and IV, history of previous surgical events, developmental or cognitive delay and psychotropic medication have been excluded.
The study population is composed of a representative sample calculated with the formula for descriptive studies for proportions, using a probability of success of 95% and a 5% failure (taken from the Jerez study) 23 in which it was described that between 40 and 60% of pediatric patients undergoing a surgical process manifest anguish; the sample consists of 97 patients.
Instrument.
The children´s manifest anxiety scale revised (CMAS-R; Reynolds and Richmond, 1985) was used, one of the most used questionnaires in childhood research. The instrument is a brief self report measure, designed as an auxiliary tool to understand and treat stress problems that affect children between 6 and 19 years of age, with a clinical approach. Values the level and nature of distress, contains 37 reagents that were answered affirmatively or negatively; obtaining a total score, in addition to four scores derived from the subscales which are physiological anxiety, restlessness-hypersensitivity, social concerns-concentration and lies. To determine a moderate to severe problem requires a standard score with a mean more than 60 (T-score), a standard deviation of 10 and a percentile above 75. 24
The CMAS-R is a test that meets the criteria of reliability, validation and standardization; developed and standardized in the United States since 1985, different versions have been developed in other languages (Boehnke, Silbereisen, Reynolds and Richmond, 1984; Ginter, Lufi, Trotzky and Richmond, 1989; Richmond and Millar, 1984; Richmond, Sukemune, Ohmoto, Kawamoto and Hamazaki, 1984; Rodrigo and Lusiardo 1992 in Spanish version for Uruguay). 24-25 the objective of the test is to obtain an accurate and valid evaluation of psychometric standards for distress such as the detection of physiological alterations, acts of hypersensitivity to environmental pressures or difficulty of concentration and interpretation.
Study description
Patients who met the selection criteria were applied the scale of manifest anxiety in children (reviewed) in the anesthesia consultation; it has been designed for patients of school-age approximately 2nd-3rd grade who have adequate reading comprehension. After signing the informed consent from the parents, the child was taken to a medical office where he read the scale to answer it individually. For the interpretation of CMAS-R, it was carried out with templates of percentile equivalents and conversions of T or scalar scores, where the total score obtained from affirmative answers were compared, converting them to scalars.
Statistical analysis
The data obtained were processed electronically creating a database, the variables used were assigned nominal data, these were described using frequency and percentages, representative graphs, and tables were made.
A descriptive analysis of all the variables included in the database was executed nominally. The discrete variables have been expressed in absolute frequencies and percentages, the continuous ones with median and standard deviations. The incidence of anxiety was described by frequencies and percentages.
Pivot tables have been calculated to establish the factors associated with anxiety, and a contingency coefficient was determined to take as significant a p <.05.
All analyses have been executed with the Stata-11 statistical package. The graphs have been plotted with Excel.
Results
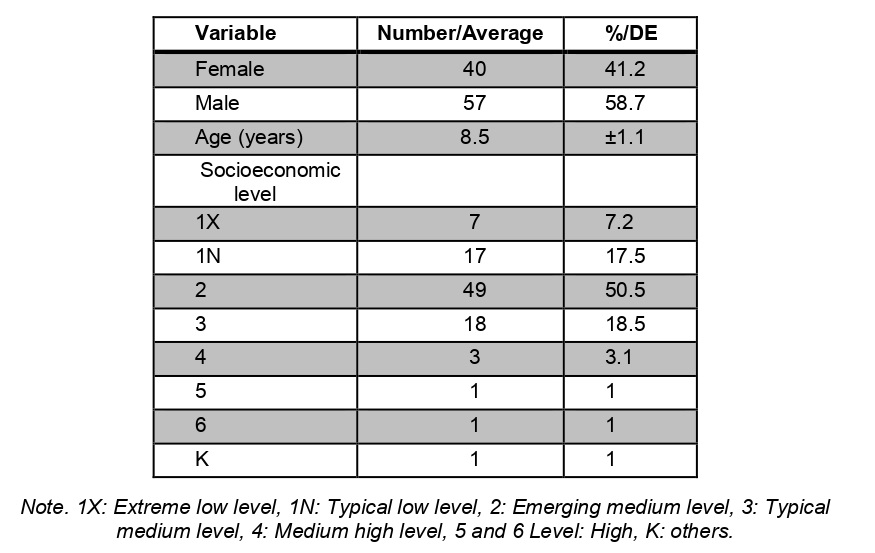
97 patients from different services that met the study criteria were included, of which 41% were female and 59% male, with an average age of 8.5 years, with a minimum of 7 and a maximum of 10 years, the prevalence was the middle socioeconomic level up to 50% (Table 1).
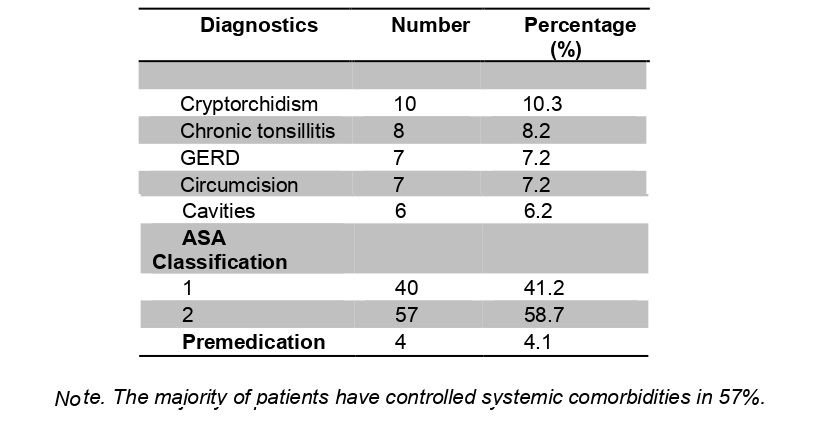
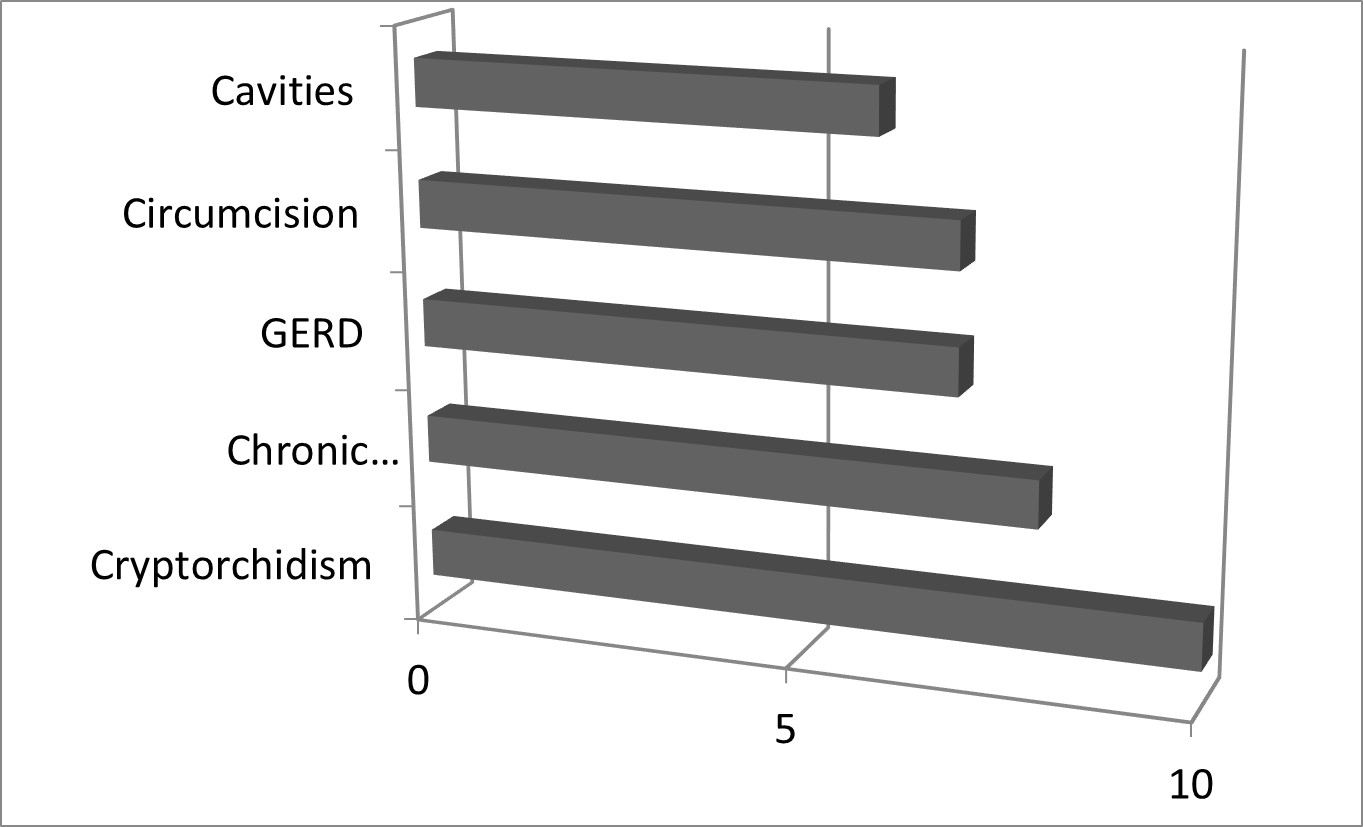
The most relevant clinical characteristics of the study patients were general pediatric surgery with a diagnosis of cryptorchidism in 10%, followed by chronic tonsillitis in 8% (Figure 2). 59% of the total patients presented with mild, controlled and non-disabling systemic disease, may or may not be related to the cause of the surgery, an anesthetic risk (ASA II) was classified (Figure 1). Only 4% of patients were premedicated. (Table 2)
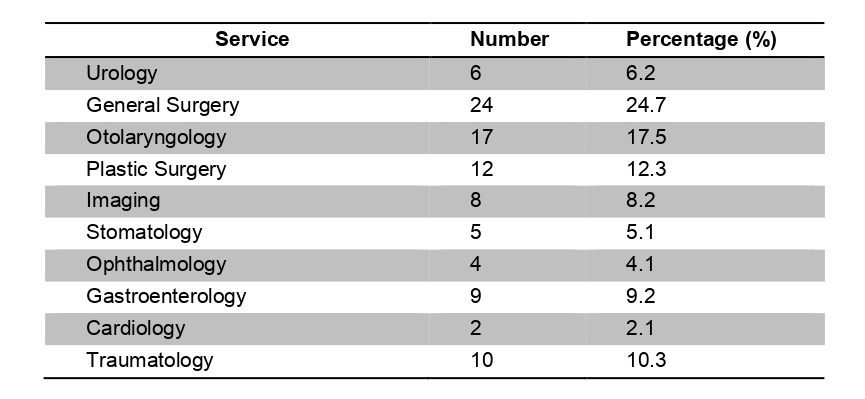
The general surgery service represents an extensive number of outpatient procedures by up to 25%, (Table 3) followed by the ENT and urology service at 17% and 12% respectively.
Regarding the use of pre-medication, its distribution corresponds to 4% while 96% of the patients did not use any drug. The most commonly used drug was benzodiazepines, as for the route of administration there is no difference intravenously or orally.
The relevant result of this study is that patients with an anxiety disorder were not detected by anesthesiologists, so they did not receive prior medication. Compared with patients who did not show any degree of anxiety, they received unnecessary drugs.
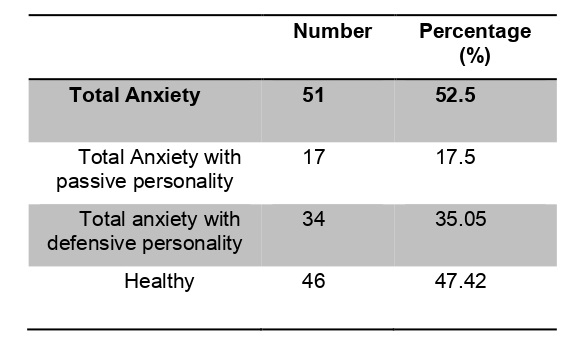
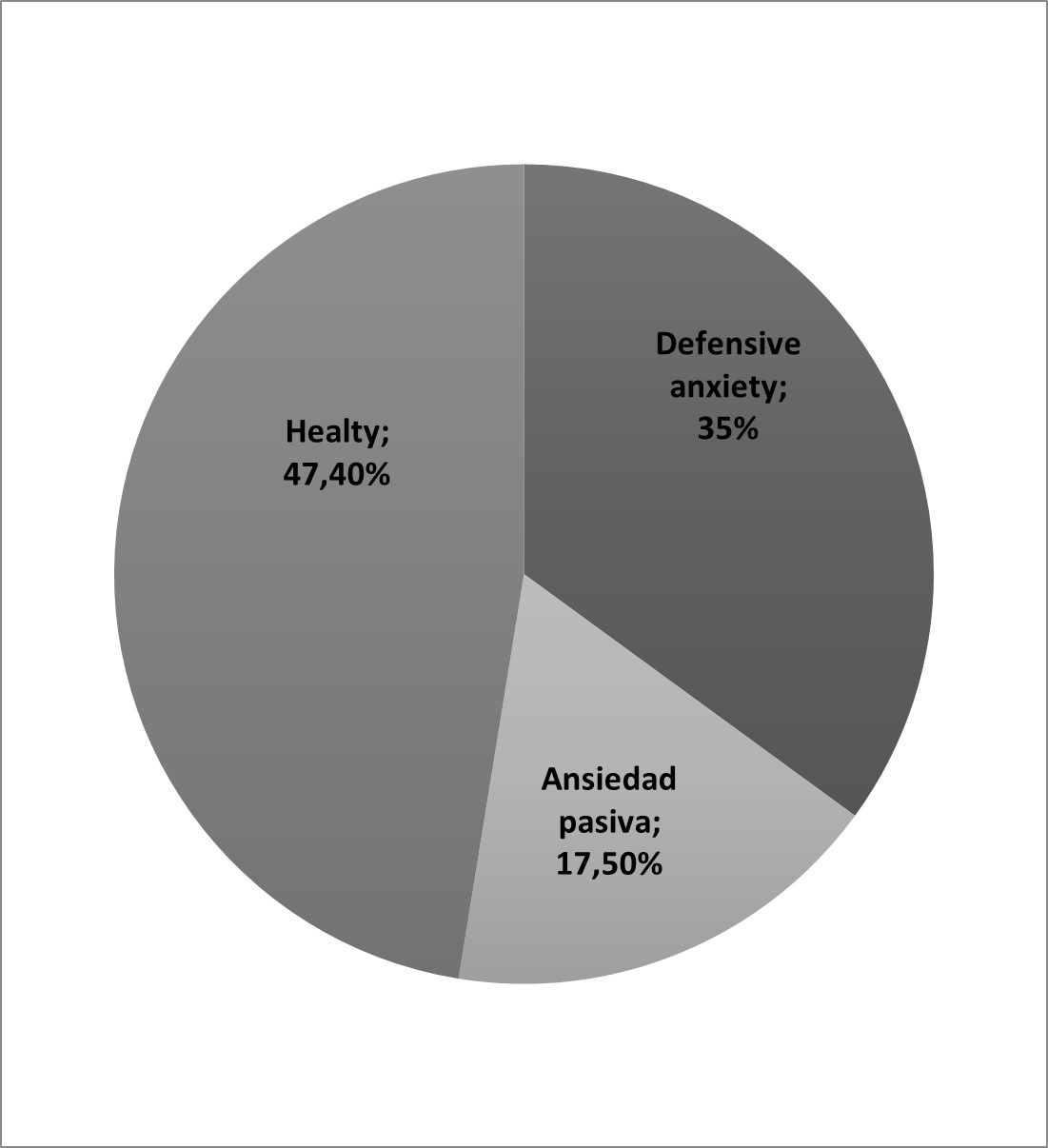
The percentage of total anxiety corresponds to 52.5% of the pediatric population, high scores suggest that the patient has experienced a moderate degree of nervousness that interferes with superior intellectual ability. Of this percentage, 35% obtained an anxiety score above the 95th percentile with a scalar score above 13 in the lying subscale, which reveals that these children, in addition to angst presented a high level of defensiveness to health personnel. The remaining 15% have a percentile greater than 95 total anxiety but a scalar score less than 13 in the lie subscale, anxiety in these patients is due to inadequate academic skills, low concept and lack of knowledge in their environment; Its described as calm and cooperative patient with difficulty in having a conversation. The rest of the patients under study did not present anxiety, restlessness or social concerns classified as healthy in 47.42%. (Table 4 and figure 3)
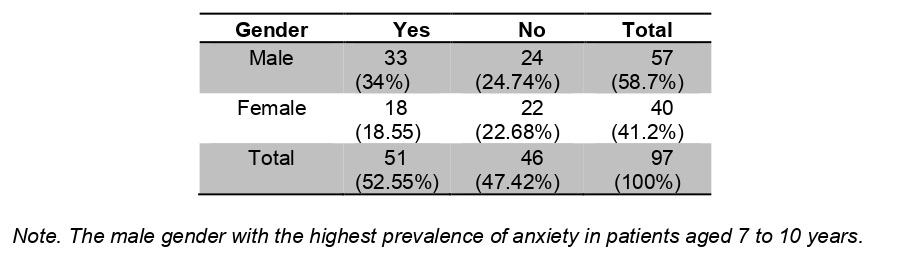
The male gender showed a higher frequency of 34% for patients who presented anxiety, while the female gender was 18.5%. (Table 5) However, gender does not show a signifying factor for anxiety in the present study (Table 5), which would require more studies to identify it.
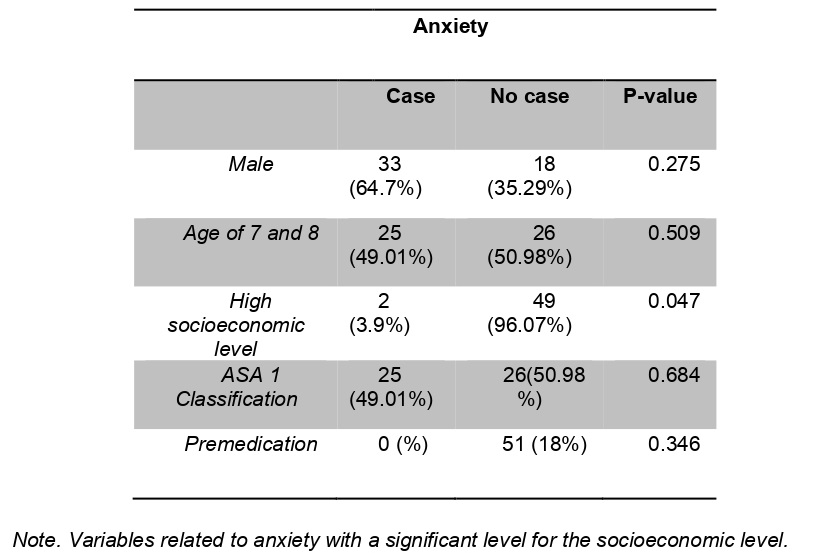
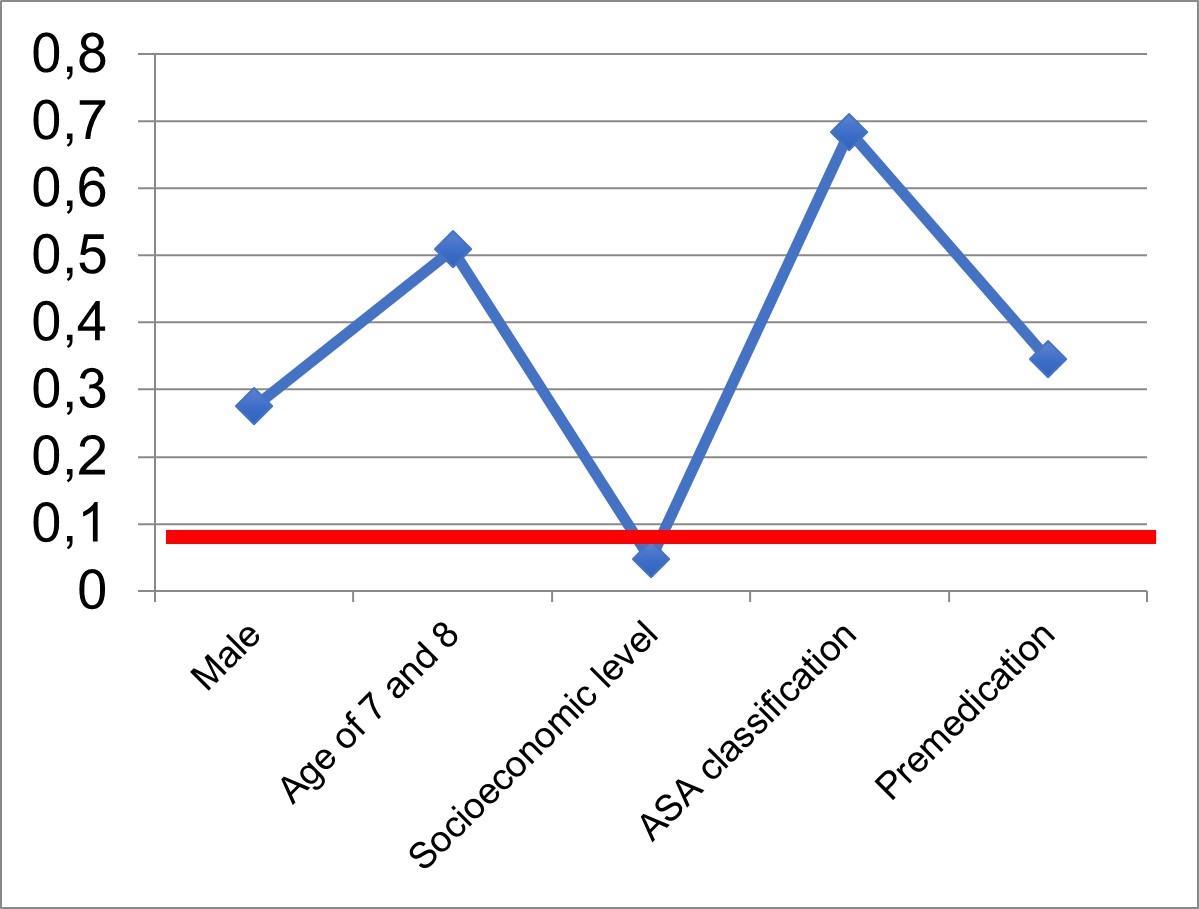
The different variables were related to anxiety; in terms of gender, we found that male patients (64.7%) presented greater frequency in total anxiety, however, their values are not significant. Regarding age and anesthetic risk (ASA), no significant results were obtained, with a p greater than 0.05 and prevalence almost 50% for the group of 7 to 8 years and 9 to 10 years. Otherwise, patients with a high socioeconomic status (3.9%) had a significantly lower frequency of anxiety than those patients with a medium or low socioeconomic status (96%), this difference being statistically significant p = 0.047 (Figure 4). Finally, none of the patients who were premedicated presented anxiety, while 52.5% of the patients who did not receive premedication presented anxiety (Table 6 and figure 4).
Discussion
In conclusion, the frequency of anxiety was 52.5% corresponding to that reported in the literature. It is important to point out the socioeconomic characteristics of the studied population, the degree of stress to which they were subjected by the parents and the use of anxiolytic drugs previously.
The clinical characteristics of the subjects studied show that most of them were male, with an ASA 2 anesthetic risk with mild controlled systemic diseases, as well as the number of procedures to which they are exposed are more than the general pediatric surgery service. There is no tendency regarding ASA for the presence of anxiety, although it has occurred more frequently in ASA 1, which explains that the subjects studied have the only pathology for which they are operated and not aggregate diseases that modify their degree of stress.
The total anxiety frequency was 52.5%; 35% of the population have a defensive personality while 15% have a passive presence and academic activity deficit. The disagreement between the expressed and the observed determines that anxiety had been underestimated and that its symptoms should not have been overlooked.
Patients with some type of anxiety were not premedicated, patients who demonstrated in the study to be healthy were premedicated with anxiolytics in 4%; in their entirety they received benzodiazepines intravenously or orally, so that the frequency of anxiety could be less than the truly expected or poorly assessed.
Age showed no influence on the presence of anxiety, however, in younger children, it would be expected that they could manifest anxiety data more frequently.
On the other hand, the socioeconomic condition had an influence on anxiety, those patients with a medium and low state had a higher incidence of angst up to 96.07% with significant values; It is consistent with what is expressed in the literature where the educational level, access to information, the father and son relationship represented at each status contributes to the presence of specific anxiety data.
The present study intends to give an initial panorama on the study of anxiety in the Institute, which would initiate a line of research in this regard, which will allow us to expand the results obtained. Due to the characteristics of the study, its objective was to determine the incidence of anxiety in the pediatric population, therefore the relationship between cause and effect or prognostic factors of this pathology has not been established.
Conclusion
In the National Institute of Pediatrics, there is a high part of children who expect outpatient surgical treatment and experience preoperative anxiety, equal to that referred to in the literature. The socioeconomic level influences the appearance of this phenomenon. The disagreement between the expressed and the observed determines that anxiety had been underestimated and that its symptoms should not have been overlooked.
The premedication of the subjects by any means is essential to reduce the manifest anxiety and the observed clinical symptoms. These results indicate the need for an evaluation with a biopsychosocial approach of children, an appropriate diagnosis of nervousness in the preoperative period, guarantees an early recovery and reduces postoperative problems.
Bibliography
1.- Perrott C., Lee C., Griffiths S., Sury MRJ. Perioperative experiences of anesthesia reported by children and parents. Paediatr Anaesth 2018 Dec;28(2):149-156. (HTML)
2.- Buffel C., Aalst J., Bangels AM., Toelen J. A web- based serios game for health to reduce perioperative anxiety and pain in children (Clinipup):Pilot randomized controlled trial. Perioperative pediatric care 2019 June; 7 (2):e12431. (HTML)
3.- Cumino D, Cagno G, Gonçalves VFZ. Impacto sobre información en la valoración preanestésica de niños y niñas con ansiedad. Rev Bras Anestesiol. 2013; 63:473−82. (HTML)
4- Weber FS. The influence of playful activities on children’s anxiety during thepreoperative period at the outpatient surgical center. J Pediatr 2010; 86:209-14. (PDF)
5- Yuki K, Daaboul DG. Postoperative maladaptive behavioral changes in children.Middle East J Anaesthesiol. 2011; 21: 183-89. (PubMed)
6- Kain ZN, Mayes LC, Wang SM, Hofstadter MB. Postoperative behavioral outcomes in children: effects of sedative premedication. Anesthesiology. 1999; 90:758-65. (PubMed)
7.- Kain ZN, Mayes LC, Caldwell-Andrews AA. Sleeping characteristics of children undergoing outpatient elective surgery . Anesthesiology. 2002 Nov. 97(5):1093–1101. (EPMC)
8.- Ahmed MI, Farrell MA, Parrish K, Aman K. Preoperative anxiety in children risk factors and non-pharmacological management. M.E.J. Anesth. 2011; 21: 154-70. (PubMed)
9.- Weaver JM, Schofield TJ. Mediation and moderation of divorce effects on children’s behavior problems. J Fam Psychol. 2015;29:39–48. (EPMC)
10- Duru E, Poyrazli S. Personality dimensions, psychosocial demographic variables, and English language competency in predicting level of acculturative stress among Turkish international students. Int J Stress Manag. 2007;14:99–110. (HTML)
11.- Suarez-Morales L, Lopez B. The impact of acculturative stress and daily hassles on pre-adolescent psychological adjustment: examining anxiety symptoms. J Prim Prev. 2009;30:335–349. (HTML)
12.- Karling M, Hägglöf B. Child behaviour after anaesthesia: association of socioeconomic factors and child behaviour checklist to the Post-Hospital Behaviour Questionnaire. Acta Paediatr. 2007;96:418–423. (HTML)
13.- Fortier MA. Kain ZN. Treating perioperative anxiety and pain in children: A tailored and innovative approach. Paediatr Anaesth, 2015 January; 25(1):27-35: 12546. (PubMed)
14.- Chieng YJS., Chan WCS., Yobas P., He HG.Perioperative anxiety and postoperative pain in children and adolescentrs undergoing elective surgical procedures: a quantitative systematic review. Journal of Advanced Nursing, 2013. 70(2):243-255. Doi:10.1111/jan.12205 (JAN)
15.- Kain Z.., Mayes LC., Caldwell-Andrews AA., Karas DE., McClain B.C. Preoperative anxiety, postoperative pain and behavioral recovery in young children undergoing surgery. Pediatrics 2006. 118(2), 651–658. (HTML)
16.- Kotiniemi LH, Ryhänen PT, Moilanen IK. Behavioural changes in children following day-case surgery: a 4-week follow-up of 551 children. Anaesthesia. 1997; 52:970-97. (HTML)
17.- Fortier MA, Del-Rosario AM, Martin SR, Kain ZN. Perioperative anxiety in children. Paediatr Anaesth. 2010;20:318–322. (PubMed)
18.- Muris P, Mayer B, Freher NK, Duncan S. Children’s internal attributions of anxiety-related physical symptoms: age-related patterns and the role of cognitive development and anxiety sensitivity. Child Psychiatry Hum Dev. 2010;41:535-48. (HTML)
19.- Davidson AJ, Shrivastava PP, Jamsen K, Huang GH. Risk factors for anxiety at induction of anesthesia in children: a prospective cohort study. Pediatr Anesth 2006;16:919–27. (PubMed)
20.- Hilly J, HorlinAL, Kinder J, Ghez C, Menrath S, Delivet H, Brasher C, NivocheY, Dahmani S. Preoperative preparation workshop reduces postoperative maladaptive behavior in children.Pediatric Anesthesia.2015; 24: 990–98. (HTML)
21.- Cagiran E, Sergin D, Deniz MN, Tanattı B. Effects of sociodemographic factors and maternal anxiety on preoperative anxiety in children. J Int Med Res. 2014;42:572-80. (PubMed)
22.- Moura LA, Guimaraes IM, Pereira LV. Prevalencia y factores asociados con la ansiedad preoperatoria en niños de 5 a 12 años.Rev. Latino –Am 2016;24:270-8. (HTML)
23.- Jerez C, Lázaro JJ., Ullán AM. Evaluación de las escalas empleadas para determinar la ansiedad y el comportamiento del niño durante la inducción de la anestesia. Revisión de la literatura. Revista Española de Anestesiología y Reanimación. 2016; 63:101-07. (Medes)
24.- Reynolds CR, Richmond BO, Tinajero Esquivel F(tr). Escala de Ansiedad Manifiesta en niños: revisada: CMAS-R.– México: Editorial El Manual Moderno; 1997. (HTML)
25- Zambrano E, Martínez JA, del Río Y, Dehesa M, Vázquez F, Zambrano M. Calidad de vida y ansiedad manifiesta en una muestra de escolares con y sin trastornos de la atención. Revista Psicología Cientifica.com. 2013; 15: 120-23. (HTML)
ACKNOWLEDGMENTS
Our sincere gratitude to the National Institute of Pediatrics for having provided its equipment and facilities to carry out the research; Dr. Minerva Dehesa Moreno for her guide to share her knowledge and experience in deciphering the appropriate anxiety scale, and Dr. Luis García for his statistical contribution in interpreting the results. Especially to all the children and their parents who have collaborated to improve the future of science.
CONFLICTS OF INTEREST.
The authors declare that they have no conflicts of interest.
INFORMED CONSENT.
Informed consent was obtained from all parents of the individual participants included in the study; the agreement was obtained by all the children.
ETHICAL APPROVAL.
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Declaration of Helsinki and its subsequent amendments or comparable ethical standards. Pediatric Ethics Committee Approval Number: 039/2016.